Many patients try to find reasons why their AF has started and look for things they do that may have initiated it. The truth however is that it is a design flaw of the mammal heart and all large mammals can get AF. AF is a condition that can occur in any of us and there are factors that make it more likely to happen. Many of these factors are out of our control like getting older, or our genes. Factors that are in our control in order of importance are being overweight, drinking excessive alcohol (>15 units a week) or being unfit. AF is also strongly associated with underlying cardiovascular problems such as high blood pressure, heart failure, coronary heart disease and valvular heart disease.
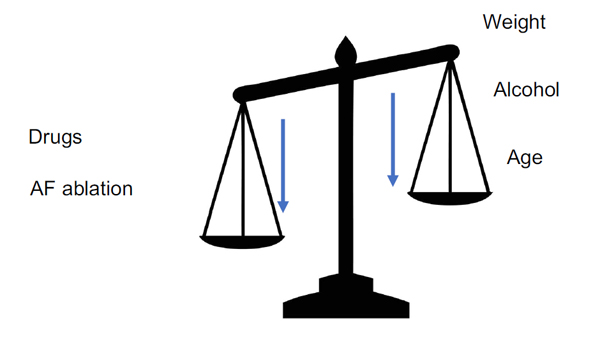
It can be helpful to think of AF risk as a balancing of scales with on one side the promoters and on the other side the reducers. As one gets older the scales gradually tip towards AF and that progress can be delayed by modifying your reversible risk factors (weight, alcohol, fitness) and having treatments like drugs and ablation. These treatments don’t cure AF, they just tip the scales back in your favour and if patients don’t take care of themselves, inevitably the AF will return as their age and reversible promoters gradually tip the scales back the other way.
Trigger and substrate
No one is sure why AF happens but it is likely that there are two factors to consider, the AF trigger and the AF substrate.
Trigger
AF is started by a trigger. Although the sinus node is usual pacemaker of the heart, all the cells in the heart have the potential to spontaneously activate. The normal heart cells are dominated by the sinus node and they activate only after they receive the electrical signal from the sinus node (link to electrical system of the heart). It is quite normal for other heart cells to occasionally activate spontaneously at the wrong time causing an ectopic (meaning in the wrong place) or extra heart beat. This is experienced as a skipped heart beat which makes the heart feel irregular for a few seconds, as opposed to AF which makes the heart feel irregular for much longer.
Occasional ectopic beats are experienced very commonly in people with normal hearts. In people who experience AF however groups of rogue atrial cells are producing ectopic beats rapidly and very frequently. These frequent ectopic beats are the trigger for AF. The rogue cells are usually grouped at the junction between the left atrium and the veins that drain blood from the lungs to the heart (pulmonary veins). It is not fully understood why the pulmonary veins are the usual location for the AF triggers and what makes the cells within the veins become active. One theory for patients with high blood pressure, where the high pressure in the heart stretches the pulmonary veins altering and distorting the atrial tissue there. Obesity may cause inflammation in the heart making these more active. However there are many people who are not obese or have high blood pressure who get AF so the story is obviously much more complex than we understand at the moment.
In patients who have otherwise normal atria the ectopic beats will initiate the AF but it soon stops on its own because the atria is not able to continually fibrillate for a prolonged period. This is called paroxysmal AF.
Substrate
The substrate for AF describes an abnormality in the electrical properties of the atrial tissue itself. In order for the multiple chaotic fibrillation waves to continually circulate around the atria they need a certain amount of room to move around. In the absence of sufficient room in they will just collide into each other and stop. A large atrium in which the electrical waves move slowly provides the ideal conditions for these perpetual waves.
By travelling slowly they leave plenty of time for the cardiac tissue to recover and become excitable so this means that the waves are more likely to always be moving towards excitable tissue. This ‘substrate’ is caused by many types of heart disease and is detectable on tests such as an echocardiogram as enlarged atria. If a patient’s heart is sufficiently abnormal then the substrate may allow the AF to be sustained without any need for the triggers described above. This is called persistent AF. Treatment of persistent AF may be more complicated because for these patients, getting rid of the trigger may not be enough to reduce the patients vulnerability to AF.
AF begets AF
It is a common story for patients to start with occasional paroxysmal AF however the attacks then become more frequent and last longer and longer until eventually the AF becomes persistent. This is because AF itself changes the electrical properties of the atria and causes the atria to dilate, in other words creates the substrate for persistent AF. Hence a term often used by doctors ‘AF begets AF’. The importance of this is that if AF is treated early on, its progression can be halted or at least postponed for many years.

